$200
Bill of materials
Designed for equitable orthopedic rehabilitation in low- and middle-income countries, where there are only 10 skilled rehabilitation providers per 1 million people.
About 374 million people worldwide suffer from knee osteoarthritis, yet global data suggests that up to 90% of individuals with chronic knee conditions never seek formal medical care.
One of the main drivers of this phenomenon is inaccessibility to orthopedic physiotherapy — the primary treatment for knee conditions. Particularly in low- and middle-income countries, there are fewer than 10 skilled rehabilitation providers per 1 million people, making these services functionally nonexistent for the majority.
Currently, there are no ways to solve this disparity in global healthcare. LMIC per-capita health expenditure routinely falls below US $200 per annum, which is well below what is needed for a standard physiotherapy program.
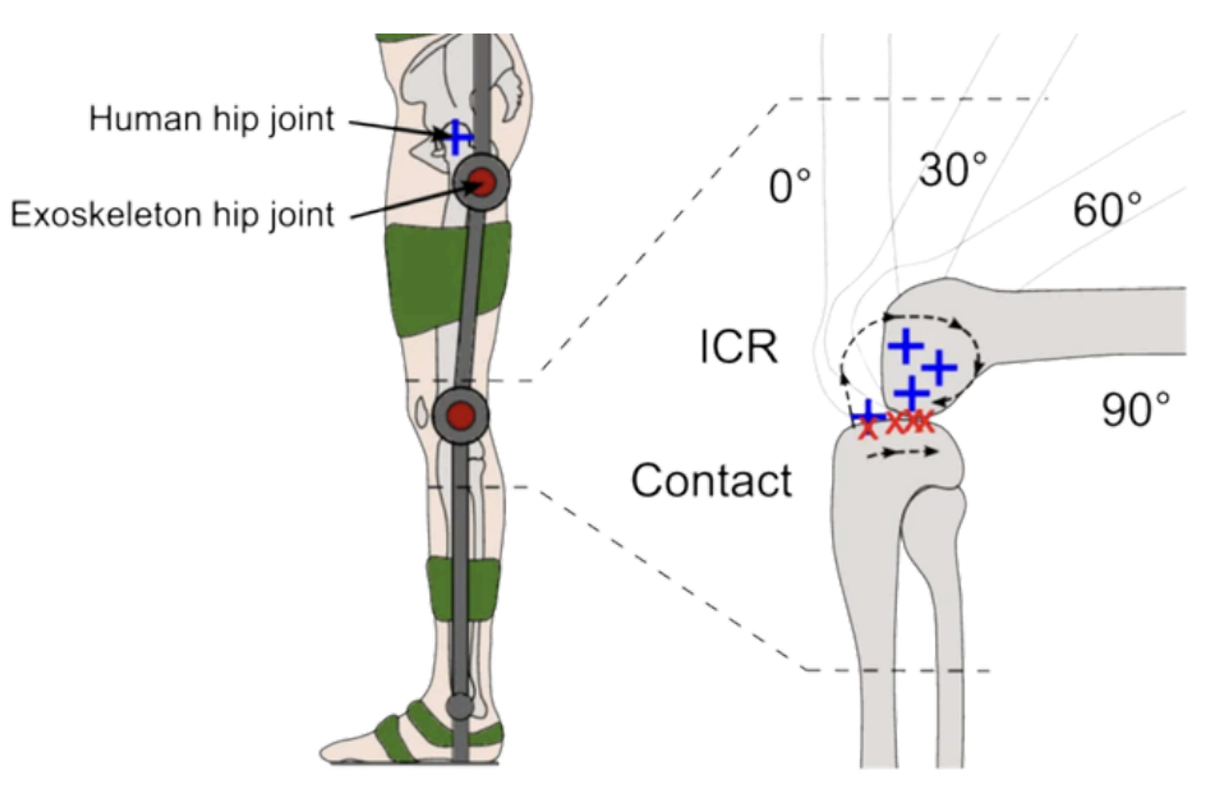
During flexion the femoral condyle rolls and slides on the tibial plateau, shifting the instantaneous center of rotation posteriorly and inferiorly. Any device built around a fixed pivot will fight the joint at every angle.
The instantaneous center of rotation (ICR) is the point about which one segment of the knee is, at that instant, purely rotating. Unlike a pin joint, the ICR is not fixed: the geometry of the condyle–plateau contact, combined with ligament constraints, traces a curve we can describe as J-shaped.
The cable's moment arm la — the perpendicular distance from the ICR to the cable line of action — is what converts cable tension into knee torque. If la collapses, so does the assistive effect. Our chain geometry is calibrated to keep la stable across the full 0°–145° range.
For real-time control, the moment arm is fitted to a fifth-order polynomial of the knee flexion angle, avoiding the cost of a per-frame analytic solve. MATLAB simulations show la decreases mildly from 0°–30°, then increases monotonically past 30° — a useful asymmetry that biases assistance toward the strenuous phases of squatting and stand-to-sit.
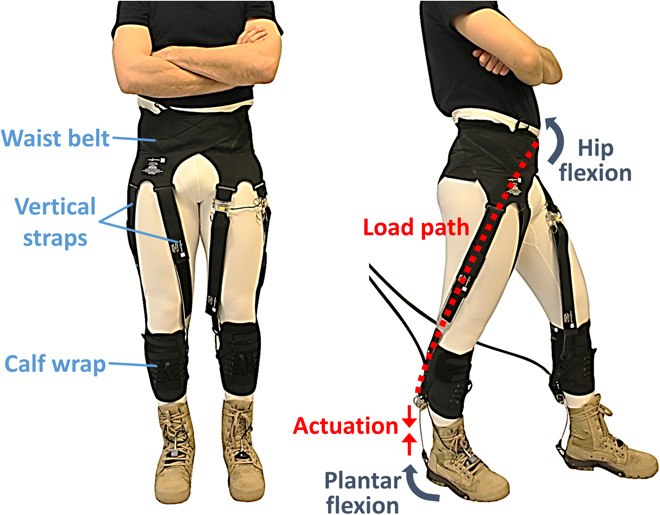
Power flows from a hip-mounted brushed-DC actuator, through a Dyneema cable, into a segmented chain wrapping the posterior knee, and out through four distributed straps that share load across the thigh and shank. The chain locks rigid only while the cable tensions; otherwise the user moves freely.
| Subsystem | Material | Mass | Position |
|---|---|---|---|
| Actuator module DH03X + gearbox + spool |
— | 380 g | hip |
| Controller cavity ESP32, BT18, LD3320, battery |
— | 220 g | hip |
| Thigh frame 2 rails + 2 cuffs |
Al 6061 + PETG | 110 g | thigh |
| Shank frame 2 rails + 2 cuffs |
Al 6061 + PETG | 95 g | shank |
| Semi-rigid chain 13 PLA links + pins |
PLA | 38 g | knee |
| Dyneema cable incl. Bowden sheath |
UHMWPE | 9 g | routed |
| Sensors 2× MPU-6050 + HX711 |
— | 12 g | limb |
| Total mass | — | 0.85 kg | — |
Eight components do everything: one microcontroller, two IMUs, one load cell, one motor + gearbox, one Bluetooth radio, one voice chip, one Dyneema cable. Each was chosen to be procurable at a community electronics market.
| Metric | Design target | Measured | Status |
|---|---|---|---|
| Cable force RMSE | < 2 N | 0.8 N | Pass |
| Knee angle RMSE | < 1° | 0.8° | Pass |
| Peak motor torque | ≥ 10 Nm | 13.5 Nm | Pass +35% |
| Battery runtime | ≥ 2.0 h | 2.2 h | Pass |
| Total mass | ≤ 2 kg | 0.85 kg | Pass · 58% under |
| Bill of materials | < US $200 | ≈ US $200 | Met |
| Donning time | < 60 s | ≤ 30 s | Pass |
| Voice command latency | ≤ 600 ms | ≤ 500 ms | Pass |
| Joint misalignment (mean) | < 5 mm | 1.39 mm | Pass · 3.6× under |
Modes switch via the mobile dashboard, Bluetooth, or the offline voice channel. Each maps to a specific clinical phase and a specific torque-or-resistance regime; the controller blends sensor signals to keep the patient inside a safe operating envelope.
The motor actively drives the cable to generate 2–10 Nm of assistive torque, smoothly modulated based on detected motion phase. The patient regains baseline ROM with minimal voluntary effort while a series-elastic element buffers transient loads.
Assistance only activates when user-generated force exceeds a configurable threshold. Encourages active participation while still catching the patient if the muscle fatigues — a moderate 3–8 Nm assist completes the motion.
Inverts the cable: the motor applies a resistive torque proportional to user effort × moment arm. Fatigue is detected via IMU signal variance; resistance backs off automatically when tremor-like oscillations exceed threshold.
Motor is passive; the device becomes a measurement instrument. Synchronized force, angle and angular velocity streams flow into the on-device analytics pipeline (07) and out to the clinician dashboard.
The analytics platform is Python + SQLite, running on the same hardware as the dashboard — a single Raspberry Pi or community-clinic laptop. Statistical and clustering modules are deterministic; only the final recommendation passes through a language model, and only after the raw signal has been compressed to a JSON summary.
{ "patient": { "id": "p_0428", "age": 42, "sex": "F", "stage": "post-ACL · week 6", "complaints": ["end-range pain", "morning stiffness"] }, "session": { "duration_s": 932, "mode": "protective", "cycles": 50 }, "statistics": { "force": {"mean_N": 182.4, "sd_N": 38.6, "p90_N": 241.0}, "angle": {"min_deg": 38.2, "max_deg": 118.7, "rom_deg": 80.5} }, "trend": { "force_delta_pct": +8.4, "rom_delta_pct": +12.1, "sessions_compared": 5 }, "clustering": { "k": 3, "silhouette": 0.62, "dominant": "moderate", "membership_pct": {"low": 14, "mod": 61, "high": 25} }, "composite_score": 74, // raw F(t), θ(t) NEVER included — privacy + tractability }
Each rehabilitation mode ran three sets of 50 flexion-extension cycles. Groups G1–G3 are identical-conditions repeatability runs; G4–G6 sweep initial angle and servo speed. Every chart below is hand-drawn from the recorded data.
Three trials under identical conditions overlay almost perfectly: peak forces 20.10, 19.60, 20.30 N (CV < 2%); minimum leg angles 52.00°, 52.50°, 52.10°; durations 40 s on the nose. The bell-shape rises from zero, peaks near t = 20 s as the cable winds in, then decays as slack returns.
The quasi-static loading at 9 °/s allows full tension to develop — the highest peak force, 20.1 N. Faster servo speeds cap tension build-up. Smaller initial angles produce higher cable forces because the leg has more travel against the moment arm peak.
Misalignment was measured against an anatomical reference at 200 equally spaced angles through the full range of motion. The distribution is sharply right-skewed: most of the mass sits below 2 mm, with a long tail toward the rapid-transition zone of mid-flexion (~ 80°–110°), where the ICR migrates most quickly.
Each session yielded one categorical AI recommendation (continue / increase / reduce / refer) and one PT recommendation, blind to each other. The diagonal of the matrix below shows agreement; off-diagonal cells were mostly adjacent (e.g. AI "increase" ↔ PT "continue"), suggesting calibration rather than category error.